
 Reviews
Reviews Why We Use CBCT: What a Cone Beam CT Reveals That X-Rays Miss
The question behind every scan: “What does the testing actually show?”
Most people who walk into a chiropractic office have been adjusted before. Far fewer have ever been shown what was wrong first. They were told something felt “out,” it got pushed back “in,” and they were asked to come back. At Koru, the order is reversed. We image before we touch, because an adjustment delivered without evidence is a guess — and the whole point of the practice is to stop guessing.
So when a patient asks what the testing actually shows, it’s a fair question. The honest answer: a cone beam CT scan turns the top of your spine from something we’d otherwise have to estimate into something we can measure, from every angle, in three dimensions. Here’s what that means in plain terms.
A Flat Picture of a Three-Dimensional Problem
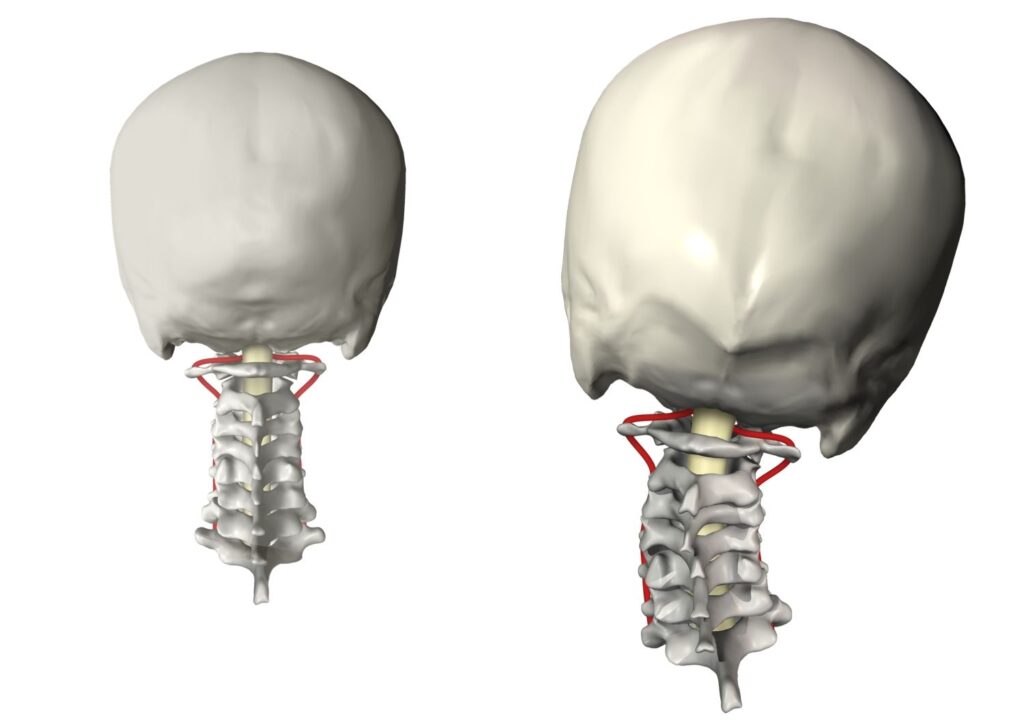
A standard X-ray is a flat shadow. It compresses a three-dimensional structure onto a two-dimensional plate, the way a hand held up to a lamp throws a single flat shadow on the wall. For a lot of the body, that’s enough. For the very top of the neck — the atlas (C1) and axis (C2) — it isn’t.
This region is small, it’s layered, and the bones overlap from almost every viewing angle. A misalignment here can be a matter of a few degrees and a couple of millimeters, in more than one plane at once. On a flat film, those planes stack on top of each other, and the true position of the bone gets hidden inside its own shadow. You can infer. You can’t precisely measure. And at the top of the neck, the gap between inferring and measuring is the gap between an adjustment that holds and one that doesn’t.
What CBCT Adds: Measuring The Atlas From Every Angle
Cone beam computed tomography (CBCT) captures the upper cervical spine as a true three-dimensional volume in a single, low-dose scan. Instead of one flat shadow, we get a model we can rotate — front, back, top, side — and slice through at any level. Nothing hides behind anything else.
That’s the difference that matters clinically. On a CBCT scan, we can see and measure the actual position of the atlas relative to the skull above it and the spine below it. We can quantify the misalignment as numbers — degrees and millimeters, in each plane — rather than a hunch. Those numbers are what NUCCA orthogonal analysis is built on: a defined model of what normal alignment looks like, and a precise account of how far a given patient sits from it.
| The short version: a 2D X-ray tells us roughly where to look. A CBCT scan tells us exactly what to correct — and gives us the measurement we’ll re-test against later to prove the correction held. |
Why The Top Of The Neck Earns This Level Of Detail
It would be overkill to scan a sprained ankle this way. The upper cervical spine is different, and the reason is anatomy. The atlas sits at the junction between the skull and the spine. Surrounding the brainstem and the structures that pass through it. When it’s misaligned, the effect isn’t limited to a stiff neck. We call the downstream picture the ASC Sequelae Framework — four specific, named effects of an Atlas Subluxation Complex:
- Postural compensation that ripples down the rest of the spine
- Altered blood flow between the brain and body
- Altered cerebrospinal fluid flow between the brain and body
- Dural tension created through the suboccipital muscles’ attachment to the dura, and therefore the brainstem
Because those effects can show up far from the neck — as dizziness, fatigue, headaches, numbness, or a low back that keeps going out — the symptom rarely points cleanly to the cause. That’s exactly why we don’t treat the symptom. We measure the structure. 3D imaging is how we see the structure clearly enough to be precise about a region where a few millimeters genuinely matter.
CBCT Above, Standing Structural X-Rays Below
A 3D CBCT answers the upper cervical question with extraordinary detail, but the spine doesn’t stop at C2. Below the upper cervical complex, we use digital standing structural X-rays for full-spine analysis under the Pierce Results System (PRS). “Standing” is the operative word: these images capture the spine under load — bearing your weight, the way it actually lives — rather than lying down, where gravity and compensation patterns relax and partly disappear.
Together, they cover the whole structure: CBCT for the three-dimensional detail of the atlas and axis, standing structural X-rays for the working architecture of everything below. NUCCA above, PRS below — both driven by what the imaging shows, not by routine. This is the part most upper-cervical-only practices don’t do, and it’s deliberate. The structure dictates the care, and the structure is the whole spine.
From Image to Correction: How a Scan Becomes a Vector
Imaging that just sits in a file isn’t worth the radiation. The point of the scan is that it produces a plan. From the measurements, we determine the specific direction and the gentle, minimum force needed to reduce the misalignment for your particular structure — what we mean when we say a correction is vector-specific. There’s no twisting, cracking, or popping for its own sake, because force is the enemy of precision. The scan tells us where, how far, and which way; the correction follows the scan.
It also gives us a baseline. Later, Comparative Re-Testing re-runs the workup against that first measurement, so “I think I feel better” becomes “here is the measurable evidence of why.” You don’t have to take our word that something changed. We show you.
The Imaging That Tells Us What We Can’t Correct
There’s a quieter reason we image first, and it’s one a lot of practices skip past. A clear picture of your structure sometimes tells us that your problem isn’t ours to solve — that what’s going on needs a different kind of care, or a referral elsewhere. We’d rather know that on day one, from the evidence, than discover it after weeks of adjustments that were never going to work.
So the scan does two jobs. It tells us what we can correct and how. And it tells us what we can’t — before you’ve committed to anything. That’s not a limitation of the technology; it’s the entire reason we trust it. We’ll tell you what we can correct, what we can’t, and what we recommend instead.
Frequently Asked Questions — CBCT Imaging in Louisville, CO
CBCT uses a low dose compared with a conventional medical CT, and we only scan when the structural question calls for it. We’ll walk you through what’s involved before anything happens, and you can ask as many questions as you want first.
A standard X-ray is a single flat image; the bones at the top of the neck overlap and hide each other on it. CBCT is a true 3D scan we can rotate and measure from every angle, which is what the upper cervical spine requires to correct it precisely.
No. We use CBCT for the upper cervical question and digital standing structural X-rays for the spine below, and only when testing indicates it. The imaging is matched to what we actually need to see.
An MRI and a CBCT answer different questions. A clean MRI means nothing is wrong with what an MRI looks for — it doesn’t measure upper cervical alignment under the model we use. A clean MRI and a structural misalignment can both be true at once.
What CBCT Is — And Isn’t
CBCT is a low-dose, three-dimensional X-ray performed on-site, on the day of your visit, with no referral delay. It is not an MRI — it’s built to show bony structure and alignment with precision, not soft-tissue pathology, and the two answer different questions. It’s also not something we run on a schedule for its own sake. We image when the structural question warrants it, and we tell you what we’re looking for before we look.
What to Expect at Koru
Every new patient at Koru begins with a detailed health history and neurological screening. When clinically indicated, CBCT cone beam imaging is taken to evaluate the craniocervical junction in three dimensions. Findings are reviewed with the patient before any care is recommended.
We serve patients in Louisville, Boulder, Broomfield, Lafayette, Erie, and the surrounding Front Range communities. No referral is required to schedule a new patient consultation.